What Would Compel an Otherwise Sane Person, or Even a Medical Doctor, to Attend a Lecture at 6:30 A.M. on a Sunday?
Novel Interventions for Low Libido
- Hormone Imbalance
Physiologically, hormone imbalance is the primary root cause of sexual dysfunction and lack of sexual desire.(1)Hormones are the engine that drives pleasure, attachment, love, orgasms, and longevity. Individuals with a balanced hormone pattern are calm, affable, enjoy high levels of trust, and intimacy.(2)
In our teens, symptoms of hormonal disruptions include acne, polycystic ovary syndrome, endometriosis, weight gain, menstrual irregularities, and premenstrual syndrome (PMS). Left unabated, in our twenties, we experience worsening PMS, infertility, hypothyroidism including autoimmune hypothyroidism, uterine fibroids, menstrual and non-menstrual pelvic pain.
Fast forward to our thirties and forties; the mirror now reflects a distinct thinning, or lack of hair, including facial hair for women, weight gain, and the beginnings of menopause.
Told that fifty is the new thirty and sixty is the new forty, it is rare amongst us who completely escape shot flashes, night sweats, sexual and or erectile dysfunction, anxiety, mood swings mid-life depression, insomnia, vaginal dryness, osteoporosis, migraine headaches, hair in places it shouldn’t be, insomnia and low libido.
Nearly all of these symptoms are due to estrogen/progesterone imbalances, testosterone insufficiencies or deficiencies and blood sugar abnormalities resulting from insulin dysregulation. To address hormonal disruptions leading to low libido, we need “CHEATO.”
The CHEAT-O THEORY
To ‘CHEAT’ when discussing hormones is to look at the “steroidogenic pathway,” the cascade of biochemical substrates and reactions necessary to produce an adequate hormone supply. (3)
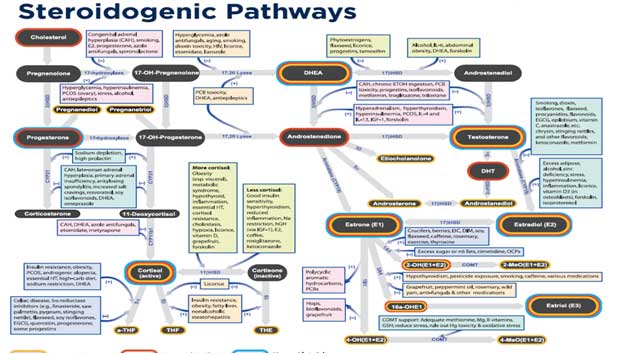
Working top-down, the “CH” represents cholesterol, the seed we’ve demonized as the root of all evil in the Western world. “E” represents the sex hormones estrogen, progesterone and testosterone, “A” is for the adrenal glands, “T” is the thyroid, and “O” is oxytocin.
Cholesterol is the primary substrate of all of the sex, steroid, and stress hormones. It is a necessary component of Vitamin D, of bile salts essential for the absorption of dietary fats and vitamins A, D, E, and K, is an integral part of cell membrane integrity, is needed for nerve and brain function, and regulates calcium metabolism and the immune response. Cholesterol is necessary for the synthesis of Coenzyme Q 10, an essential component of cell respiration responsible for producing cellular energy, is needed for neuroregeneration of damaged nerve and brain tissue and is a building block for Vitamin K2, an essential cofactor for hepatic synthesis of blood-clotting proteins.
Estrogen, the dominant hormone in the first half of a woman’s menstrual cycle has some 400 identified functions in the body. Estrogen affects metabolic rate, insulin sensitivity, body temperature, muscle maintenance, sleep, and blood flow to the brain. Natural estrogen decreases the incidence of blood clots, accumulation of arterial plaque, and preserves collagen in the skin.
There are three types of estrogen. E1 (Estrone)is the prominent post-menopausal estrogen. High levels of estrone increase breast cancer risk. 25 mg. of 7-Keto DHEA, on average will decrease estrone by 50%.
E2 (Estradiol) is the most potent estrogen. Estradiol acts an antioxidant, increasing “good” cholesterol (HDL), while reducing triglycerides, LDL and total cholesterol. E2 aids in memory preservation (by increasing serotonin levels in the brain), aids in maintaining bone structure, and aids in the absorption of calcium, magnesium, and zinc.
E–3 (Estriol)is the least powerful, most beneficial component of the three. E3 acts to protect against breast cancer, (4) maintains pregnancy, controls the symptoms of menopause, decreases LDL and increases HDL. Used for relief of postmenopausal atrophy, topical E-3 also impacts vaginal dryness and urinary incontinence. It does not have the brain, bone, or heart protection of estradiol.
When estrogen is in excess, think “cysts” of the affected organs. Fibrocystic breast disease, uterine fibroids, ovarian cysts, and endometriosis are the result of estrogen dominance. Heavy menstrual bleeding including postmenopausal spotting, breast tenderness, insulin resistance, weight gain, depression,and reduced libido are all symptoms of estrogen accumulation.
Estrogen deficiency presents as hot flashes, night sweats, brain fog, belly fat, memory loss, thinning hair, skin and nails, osteoporosis, vaginal dryness, and low libido.
Progesterone balances estrogen, acts as “nature’s valium,” having a natural calming effect, lowers blood pressure, lowers LDL (“bad”) cholesterol, is anti-inflammatory, thickens scalp hair, protects against breast cancer, coronary artery disease, and osteoporosis, promotes immunity, enhances thyroid function and improves libido.
Progesteroneexcessresults in weight gain increased cholesterol, fatigue, depression, sugar cravings, bloating, fullness, constipation, urinary incontinence, decreased libido, breast or nipple tenderness, and immune suppression.
Progesterone is the first of the female sex hormones to decline as a patient enters menopause. Deficiency symptoms include anxiety, depression, severe insomnia, osteoporosis, weight gain, irritability, headaches, the feeling of wanting to jump out of one’s skin, and reduced libido.
Testosterone in men and women increase muscle mass and strength, decreases excess body fat, maintains cognition and memory, increases sexual interest, libido and performance prevents bone deterioration, and elevates norepinephrine in the brain, rendering testosterone a powerful antidepressant.
In excess Testosterone causes acne, anxiety, anger, agitation, hair‐loss, male‐pattern baldness, infertility, insulin resistance, weight gain, edema, high blood pressure, oily skin, oily hair and breakouts on the neck and shoulders.
Testosterone deficiency appears as apathy and fatigue, headaches, poor muscle tone, decreased libido, thin lips/saggy cheeks, trouble with orgasm, depression,and urinary incontinence.
Statin use is associated with significantly lower serum total and non-SHBG-bound
testosterone levels. (5)
The Adrenal Glands, pea-sized organs, sitting atop of the kidneys, produce hormones that regulate blood pressure, electrolytes balance, blood sugar, immune responses, digestion, and stress responses.
Constant, unremitting stress, an everyday occurrence in society, hijacks normal hormonal responses, redeploying the adrenals’ resources to combat the “evil” of the moment. The other adrenal functions, digestion, immune response, and especially thyroid hormone production, are temporarily put on hold or slowed until the issue has passed.
In an ideal world, the stress passes quickly, and the adrenals resume their business. In our non-ideal, one stress begetting another stress, begetting the third stressor, ad infinitum world, puts our adrenal glands into overdrive. Cortisol floods the body driving the adrenals to handle the pressure but eventually, unable to keep up,ends in a “burnout” type of fatigue.
Cortisol, produced in the adrenal glands, is our emergency “fight or flight,” protector hormone. When danger lurks, cortisol brings the body to a state of heightened awareness. When the threat passes, in theory, circulating cortisol levels drop to near zero waiting for the next emergency signal.
In our non-idealized world, cortisol levels never decrease to their subclinical levels, acting as a rogue warrior, sending out aberrant signals. Cortisol displaces the other hormones, notably thyroid hormone.
Symptoms of hypercortisolemia include a fatigue pattern with a distinct daily energy pattern. Our patient experiences difficulty rising early in the morning, never feeling fully awake until 10 AM. She needs a “pick me up,” coffee, tea, an energy drink, shortly after that. She feels as if she has not slept at all. Her best, most refreshing sleep comes between 7-9 AM. (6)
After the noon meal, the patient feels better and fully awake only to suffer an energy drop with a need for a nap between 2 and 4 PM. Her worst time of the day is the dinner hour between 5- 7 P.M. She can barely make it to the couch. Working the remote on the TV is the extent of her exercise routine. Between 9 and 11 PM, curiously, she gets a burst of energy and is most productive in working and playing. There is often a resistance to going to bed with a second burst of energy after 11 PM occurs lasting until 1-2 AM. Sleep is fitful, and the pattern recurs unless someone does an intervention.
DHEAproduced in the adrenal glands, brain, and skin, is nicknamed “the mother of the steroid hormones.” A precursor of testosterone and estrogen regulates mood supports the immune system, improves insulin sensitivity and is essential to bone health, and weight loss.
DHEA increases one’s sense of wellbeing, aids in the repair of tissue, alleviates allergic reactions, increases brain function, lean body mass lowers triglycerides, and helps prevent blood clots. It plays a role in improving insulin sensitivity and preventing adult-onset diabetes. (7)
It enhances sex drive and desire, skin tone, reduces cellulite, clitoral and vulvar vaginal atrophy in postmenopausal with no systemic effects (8).
Low levels of DHEA are associated with all-cause mortality, cardiovascular mortality, immune dysfunction, autoimmune disease, cancer, hypertension, cardiovascular disease, depression and loss of well-being, low libido, erectile dysfunction, burning mouth syndrome, neurodegenerative disorders, hypothyroidism due to an inability to convert T4 to T3, bullous pemphigus, psoriasis and osteoporosis. (9)
A high Cortisol to DHEA Ratio (Normal Cortisol/DHEA <6/1) is indicative of an active depressive state. By lowering the cortisol/DHEA ratio, her depressive state lessens.
DHEA replacement in women increases testosterone levels.(10)
DHEA administered to physiologic values significantly impacted Female Sexual Arousal Disorder (FSAD). Compared to placebo arousal/ sensation was improved by 68% (P = 0.006), arousal/lubrication by 39% (P = 0.014), orgasm improved by 75% (P = 0.047), and dryness during intercourse by 57%. (11)
A butterfly-shaped organ, located in the laryngeal prominence, or Adam’s apple, the thyroid gland, acts as our gas pedal, determining how fast or slow every cell of our body operates. The thyroid is responsible for the smooth functioning of the heart, lungs, G.I. tract, blood sugar, cholesterol production and utilization, bone metabolism, blood, brain function and adequate and timely production of hormones.
An estimated 12 percent of the U.S. population will develop a thyroid condition during their lifetime. Sixty percent of those patients are symptomatic but unaware of their situation. (12) Nearly all patients present with low (hypothyroid) thyroid production.
Symptoms of hypothyroidism include cold intolerance, unexplained weight gain, fatigue, thinning of the hair, the outer third of the eyebrow, dry skin, cracking nails, increased body fat, energy loss, cognitive loss, memory loss, mood disorders, lowered body temperature (never higher than 97.6 F), fluid retention, and a reduced sense of well-being are all attributable to poor thyroid function.
Hyperthyroid symptoms are the mirror opposite: Warm, moist skin, unexplained weight loss, elevated body temperature, palpitations, diarrhea, tremors, difficulty sleeping, a sense of “jumping out of one’s skin,” hair loss, bulging eyes, muscle weakness, and scant periods.
The thyroid is a “Goldilocks” hormone. It needs to be not too little, not too much, but just right. In men, both hypo and hyperthyroidism lead to erectile dysfunction. In women, dyspareunia, painful intercourse is the issue. In both genders low libido is common.
Oxytocin, synthesized in the posterior in the hypothalamus and secreted by the posterior pituitary gland, increases pleasure, attachment, love, orgasms, and longevity. Individuals with high oxytocin levels are calm, affablyjoyo us in their activities of daily living, and enjoy high levels of trust.(13)
Oxytocin increases with food intake, soft-touch, massage, reading, viewing pictures of loved ones, music, singing, physical exercise, positive environments, positive social contacts, living with others, partner support, mother’s love, romantic love, and orgasm.
Dr. Paul Zak, the self-styled “Love Doctor,” recommends, to increase oxytocin, eight hugs per day. (14)
Oxytocin controls sexual function. DHEA&testosterone control sex drive and desire. (15)
Oxytocin produces nitric oxide, a blood vessel dilator with action similar to phosphodiesterase type 5 (PDE5) inhibitors, sildenafil (Viagra) and tadalafil (Cialis).
Oxytocin deficiency is present in postmenopausal women with estrogen deficiencies, hypothyroidism, usually low T3, depression, AIDS, CMV infections, Multiple Sclerosis, fibromyalgia, chronic stress situations, chronic opioid use, Parkinson’s Disease, loneliness, anxiety, fear, and certain types of schizophrenia. (16)
To determine oxytocin status, we ask individuals to rate themselves on happiness, feelings for others, social interactions, love, touch, muscle-tendon pain, sexual desire and performance, their degree of social interaction or isolation, and even whether their world is a bright and cheery or a cold, uninviting place.
Evaluation
History Physical /Testing
Medical / Surgical / Social / Family history / Gynecologic
Comprehensive symptom checklist
Pap, BMD, Colonoscopy (age dependent)
Baseline testing needed:
CBC, CMP, CRP, Homocysteine, Lipid Profile
25 Oh-Vit D3
Hemoglobin A1C, Fasting Insulin
Thyroid-TSH, free T3, free T4, rT3, TPO, Antithyroglobuliin, TSI (if S/S/ indicate), ferritin
Hormones-Estrone, Estrogen, Progesterone, Testosterone (Day 19-21 if Premenopausal)
E/P Ratio =E1+E2/P Goal <250
P/E Ratio=Px 1000/E Goal 100-500
As Indicated
Cortisol (Serum, Urine, Saliva)
DHEA-S, IGF-1
Oxytocin; Oxytocin Challenge Test
Hormonal Effects on Libido
| Hormone | Effect | Effect of Deficiency |
| Cholesterol | Substrate necessary for the production of sex hormones | Low testosterone
Low libido, sexual desire |
| Estrogen | Enhances Blood Flow to Brain
IncreasesHDL Maintains Vaginal Tissue |
Hot Flashes
Night Sweats Brain Fog, Dementia Osteoporosis |
| Progesterone | Increased Sexual Desire
Calming Improved Sense of Well Being
|
Poor Libido
Agitated, Irritable Insomnia Weight Gain Depression |
| Testosterone | Directly Responsible for:
Sex Drive, Sexual Desire Vaginal Lubrication |
Apathy, Depression
Poor Libido Poor sexual performance |
| Adrenal Gland-Cortisol | Stress Response
Energy Production Production of Leutinizing Hormone (LH) Testosterone Precursor |
LH Suppression =
Testosterone Deficiency Fatigue, “Burn-Out” Sugar Cravings |
| DHEA | Sexual Drive and Desire
Precursor Substrate: Testosterone Estrogen |
Erectile Dysfunction
Poor Libido Hypothyroidism Depression |
| Thyroid | Sexual Performance
Sexual Desire |
Erectile Dysfunction (Males)
Dyspareunia (Female) |
| Oxytocin | Sexual Function
Pleasure |
Fear
Loneliness Isolation |
| Prolactin | Mediates Sexual Satisfaction | Male:
Impotence Decreased Sperm Decreased Libido Decreased testosterone Female: Amenorrhea Decreased ovulation Diminished Libido |
References
- https://www.issm.info/sexual-health-qa/do-men-suffer-from-low-libido/
- Hertoghe, T. Passion, Sex, and Long Life – the Incredible Oxytocin Adventure. ISBN 978-2-9599713-4-1, January 2010, Luxemburg, by International Medical Books/Archimedial, 4B Route d’Arlon, L-8399, Windhof, Luxembourg.
- https://www.google.com/url?sa=i&source=images&cd=&cad=rja&uact=8&ved=2ahUKEwjJyq6EgqDgAhVECKwKHYczA2gQjRx6BAgBEAU&url=https%3A%2F%2Fwww.pinterest.com%2Fpin%2F392868767486143454%2F&psig=AOvVaw2emdnu9r2S4HpteS8KT7Dr&ust=1549298750778456
- Gordon, Mark L. Principles of Interventional Endocrinology. Physician’s Guide to Anti-Aging and Regenerative Medicine; 2009, 1 (74-75)
- Catherine E de Keyser, Filipe Valerio de Lima1, Frank H de Jong, Albert Hofman, Yolanda B de Rijke, Andre´ G Uitterlinden, Loes E Visser and Bruno H Stricker; “Use of statins is associated with lower serum
total and non-sex hormone-binding globulin-bound testosterone levels in male participants of the Rotterdam Study, European Journal of Endocrinology, 173:2 155–165
- Metcalf, Eric, http://www.webmd.com/a-to-z-guides/features/adrenal-fatigue-is-it-real, Accessed February 16, 2015
- Roden, E et al.,”A Medical Progress: Risk of Testosterone replacement therapy and recommendations for monitoring,” NEJM 2004; 350:482-492
- Ohisson C, et al. Low Serum Levels of Dehydroepiandrosterone Sulfate Predict All-Cause and Cardiovascular Mortality in Elderly Swedish Men. J Clin Endocrinol Metab. 2010 Jul 7.
- Kritz-Silverstein, D et al. Effects of DHEA supplementation on cognitive Function and Quality of Life: The DHEA and Well-Ness (DAWN) Study. J Am Geriatric Soc. 2008 July; 56 (7)
- Huber, G, Bioidentical Hormones. Module 1 A4M, Presented Dec. 12, 2015; 15
- Genazzani AR, Stomati M, Valentino V, Pluchino N, Pot E, Casarosa E, Merlini S, Giannini A, Luisi M. Effect of 1‐year, low‐dose DHEA therapy on climacteric symptoms and female sexuality. 2011 Dec;14(6):661‐8
- General Information, Press Room, http://www.thyroid.org/media-main/about-hypothyroidism/, Accessed July 5, 2015.
- Hertoghe, T. Passion, Sex, and Long Life – the Incredible Oxytocin Adventure. ISBN 978-2-9599713-4-1, January 2010, Luxemburg, by International Medical Books/Archimedial, 4B Route d’Arlon, L-8399, Windhof, Luxembourg.
- Zak, Paul, Trust, Morality and Oxytocin, TED Talks, https://www.youtube.com/watch?v=rFAdlU2ETjU, November 1, 2011, Accessed March 25, 2015.
- Flechas, Jorge, and Hertoghe, T., Assessing Oxytocin Deficiency in Your Patients, http://cabecahealth.com/articles/assessing_oxytocin_sufficiency.pdf, Accessed March 29, 2015
- Flechas, Jorge, and Hertoghe, T., Assessing Oxytocin Deficiency in Your Patients, http://cabecahealth.com/articles/assessing_oxytocin_sufficiency.pdf, Accessed March 29, 2015