Pellet Therapy
A Premier Choice for Long-Lasting Hormone Balance and Vitality
🌿 A Smarter Solution for Women Over 40
If you’re feeling the effects of hormonal shifts—fatigue, mood swings, brain fog, weight gain, or loss of libido—you’re not alone. Hormonal imbalance can quietly erode your quality of life. At Clearfield Medical Clinic, we offer a modern, effective solution: bioidentical hormone pellet therapy.
💡 Why Pellet Therapy?
Pellet therapy is a convenient, low-maintenance way to restore hormone balance. Unlike creams or injections that require daily attention or weekly appointments, pellets provide a consistent, time-release delivery system—so you don’t have to think about your hormones every day.

🌿Pellet therapy
- Requires only 3–4 procedures per year
- Eliminates hormone fluctuations
- Avoids risks like skin transfer (common with creams) and injection-site discomfort
🌟 The Benefits of Pellet Therapy
Women in Reno are choosing pellet therapy for its reliability and noticeable results. Benefits include:
- ✅ Stable Hormone Levels for 4–5 months
- ✅ Relief from hot flashes, night sweats, and mood swings
- ✅ Increased libido, energy, and focus
- ✅ Improved memory, bone density, and metabolism
- ✅ Plant-derived and bioidentical to your body’s natural hormones
- ✅ No increased risk of blood clots (unlike synthetic oral estrogens)
🔬 What Are Pellets, Exactly?
Hormone pellets are tiny cylinders, custom-compounded from bioidentical estrogen or testosterone. Sourced from plants and structurally identical to human hormones, these pellets are placed just under the skin in a quick, in-office procedure.
Once inserted, they deliver a steady stream of hormone support, mimicking the way your ovaries or testes once functioned.
✅ FDA Note: Testosterone pellets (75 mg) have been FDA-approved since 1972 for hormone replacement.
🏥 Why Clearfield Medical Clinic?
Dr. William Clearfield has over two decades of experience in bioidentical hormone optimization. At our Reno clinic, pellet therapy is one of our most popular, patient-approved methods—offering a practical and proven way to regain control of your health.
✨ Rediscover the Best Version of You
If menopause, perimenopause, or low testosterone are affecting your mood, energy, sleep, or intimacy—pellet therapy may be your answer.
Schedule a consultation today and experience the Clearfield approach to safe, customized hormone balance.
🌿What Are Hormone Pellets?
Long-Lasting, Natural Hormone Delivery
Bioidentical hormone replacement pellets are tiny, rice-sized cylinders crafted from plant-based estrogen or testosterone. Custom-compounded by a certified pharmacy for Clearfield Medical Clinic, these pellets are inserted just under the skin to provide a steady, consistent hormone release for 3–5 months in women and 4–6 months in men.
✅ FDA-approved since 1972, testosterone pellets have a long-standing safety profile.
✅ Pellets maintain stable hormone levels, avoiding the peaks and crashes of creams, patches, or injections.
✅ Unlike synthetic hormones, bioidentical pellets carry no increased risk of blood clots.
🌿 Key Benefits:
- Relief from menopause and andropause symptoms
- Enhanced libido, energy, mood, and sleep
- Improved bone density, memory, and urinary health
- Reduced migraines and menstrual headaches in women
- Increased strength and mental clarity in both sexes
At Clearfield Medical Clinic, pellet therapy is our preferred method due to its unmatched convenience, safety, and effectiveness.
✨Why Pellet Therapy Is Virtually Painless
Precision Technique, Minimal Discomfort
Dr. William Clearfield’s background in emergency medicine led him to refine a nearly pain-free pellet insertion technique.
Before insertion:
- A topical anesthetic cream is applied
- Followed by cold spray and local Lidocaine to ensure full numbness
The procedure:
- Takes under 2 minutes for women, and less than 4 minutes for men
- Involves a small incision and a quick, simple pellet insertion
- Is followed by a steri-strip and clear dressing
- Leaves minimal to no scarring and rarely causes discomfort
Most patients say it’s faster and easier than a blood draw—and the benefits last for months.
🌿Managing Pellet Therapy Side Effects & Complications
What to Expect—and How We Prevent Problems
🩺 Insertion-Related Issues (Rare):
- Minor bleeding, bruising, or skin discoloration
- Temporary discomfort or pellet extrusion (extremely rare)
- Infection (mitigated by single-use, sterilized insertion kits)
Note: Since returning to our trusted instrument supplier two years ago, no pellet extrusions have occurred.
🧬 Hormonal Side Effects:
Excess Testosterone
May cause:
- Oily skin, acne
- Temporary increase in facial hair in women
- Rarely, mood swings or headaches Managed with:
- Supplements, medications, or dietary changes (e.g., reishi, red clover, chasteberry, maca root, saw palmetto)
- Spironolactone, a potassium-sparing diuretic that blocks excess testosterone effects
🧬Estrogen Excess
May cause:
- Breast tenderness, mood swings
- Vaginal bleeding or water retention
- Gynecomastia in men
Treated with: - Progesterone supplementation
- Herbal support (chrysin, DHEA, pregnenolone)
- In rare cases, anastrozole (an estrogen-lowering medication)
Increased Red Blood Cell Count (Men)
Testosterone can raise red blood cell production.
If hemoglobin >18.5 or hematocrit >55, a blood donation is recommended.
⚠️ Post-Insertion Guidelines:
- Avoid strenuous exercise or heavy lifting for 48 hours
- No hot tubs, saunas, or pole dancing (yes, seriously)
- A low-dose antibiotic is prescribed for immunocompromised or joint replacement patients
🌿Pellet Therapy, Cancer Risk & Additional Benefits
What the Research Says About Safety
Far from increasing risk, testosterone therapy may reduce breast cancer incidence by up to 50%.
📊 One study of 1,268 women showed:
- Breast cancer rates of 142 per 100,000 in the testosterone pellet group
- Compared to 390 per 100,000 in the control group
✅ Safe for Breast Cancer Survivors
In a study of 43 breast cancer survivors using a combo of bioidentical testosterone (60 mg) and anastrozole pellets every 90 days:
- 93% achieved optimal hormone levels
- No cancer recurrence or significant side effects over 3 years
- Some with metastatic breast cancer showed no disease progression
🚺 Safe Hormones for Women:
- Bioidentical progesterone and estriol have shown no increased cancer risk
- Estriol, used widely in Europe, may actually reduce recurrence and mortality risk
💇♀️ Bonus Benefit: Better Hair & Skin
Pellet therapy can improve scalp hydration, reduce hair thinning, and restore skin tone and elasticity—all by correcting underlying hormone imbalances.
⏱️ Onset & Duration
- Most patients feel the benefits within 4–7 days
- Pellets last 3–5 months for women and 4–6 months for men
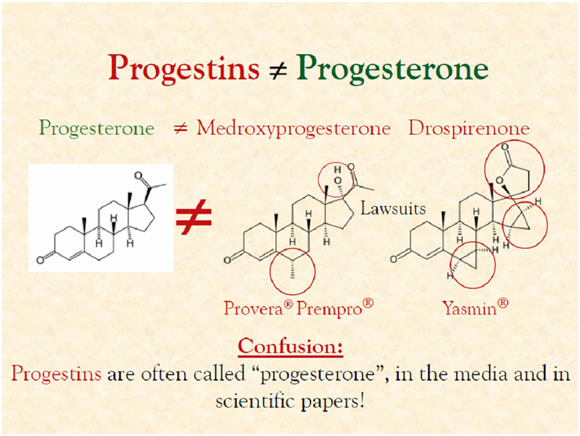
🌿What About Progesterone?
Estrogen’s Essential Partner in Hormone Balance
Let’s rewind to 1979. Metropolitan Hospital, Philadelphia. (It’s a condo now—bad management, not my fault.) I’m Dr. Bill, a young OB/GYN resident. Like many gynecologists of the era, I performed lots of hysterectomies. Post-op, we routinely prescribed synthetic, horse urine-derived estrogen to prevent hot flashes.
We didn’t prescribe progesterone. We used Provera, a synthetic progestin—which is not the same as natural progesterone. We believed progesterone’s only job was to prevent uterine lining stimulation from estrogen. Since these women had no uterus, we thought it was irrelevant. We were wrong.
🔬 What We Know Now:
Natural progesterone plays a far broader role. It has receptors in the:
- Brain
- Heart
- Breast
- Bone
- Bladder
- Uterus
It helps regulate mood, protect breast tissue, support bone density, and counterbalance estrogen’s proliferative effects.
💊 Forms of Progesterone Therapy:
- Oral capsules (e.g., Prometrium®, FDA-approved in 1998)
- Topical creams
- Vaginal formulations
- Compounded custom doses
Note: Progesterone pellets are not currently a reliable delivery system, due to absorption variability.
🔁 Dosing Guidelines:
- Premenopausal women cycle progesterone on days 14–25 of the month
- Dosing depends on symptoms and labs:
- Oral: 6.25–250 mg
- Transdermal: 3–30 mg
Only oral (100–200 mg) and vaginal (45–90 mg) progesterone protect the uterine lining from estrogen stimulation.
🌿 Other Pellet Therapy Indications:
Pellet therapy treats more than just menopause symptoms. It’s also effective for:
- Severe PMS
- Postpartum depression
- Menstrual migraines
- Sleep disorders
- Sexual dysfunction
- Hormonal suppression from birth control
🌿Hormone Monitoring – Why Testing Still Matters
Personalized Care Begins With Data
Every patient at Clearfield Medical Clinic undergoes comprehensive lab testing before starting hormone therapy. We evaluate serum hormones, and when on pellets, we also monitor saliva levels and symptom changes to fine-tune treatment.
👨⚕️ A Cautionary Tale: David, Age 70
David was referred by a psychologist for fatigue, low libido, muscle weakness, and loss of motivation. The referral slip read: “Treat with testosterone.”
Seems logical—except his labs showed:
- Total testosterone: 700 ng/dL (excellent)
- Free testosterone: 14 pg/mL (normal for a man half his age)
After further investigation, we diagnosed acute lymphocytic leukemia. Had we followed the referral blindly, testosterone therapy could have worsened his condition. As Egon from Ghostbusters said, “Crossing the streams is bad.” Very bad.
🧪 Monitoring on Pellet Therapy
Pellets can suppress or distort serum hormone readings. Therefore, we:
- Monitor symptoms + saliva levels after the first insertion
- Repeat labs before each new pellet insertion during the first year
- Then 1–2 times per year thereafter
🌿The Final Word on Pellet Therapy
Bioidentical hormone pellets are a safe, effective, and convenient option for both women and men. They deliver consistent hormones with minimal hassle and no daily maintenance.
Pellet therapy has been shown to:
- Improve bone density
- Enhance sexual function
- Elevate mood, memory, and cognition
- Reduce urinary incontinence
- Alleviate vaginal dryness
- Improve lipid profiles and cardiovascular risk
- Optimize hormone metabolism and detox pathways
Whether you’re navigating menopause, andropause, or simply want to age with energy and clarity—pellets provide a stable, predictable hormonal environment for lasting wellness.
🌿References
- Jockenhövel J, et al. Pharmacokinetics of Subcutaneous Testosterone Implants in Hypogonadal Men. Clin Endocrinol. 1996;45(1):61–71.
- Handelsman DJ, et al. Analysis of Testosterone Implants for Androgen Replacement Therapy. Clin Endocrinol. 1997;47(3):311–316.
- Glaser RL, Dimitrakakis C. Reduced Breast Cancer Incidence in Women Treated with Subcutaneous Testosterone or Testosterone + Anastrozole. 2013;76(4):342–349.
- Glaser RL. Subcutaneous Testosterone-Anastrozole Therapy in Breast Cancer Survivors. ASCO Breast Abstract 221, 2010.
- Pastuzak AW, et al. Pharmacokinetics and Dosing of Testosterone Pellets. 2012;33(5):927–937.
- Morgentaler A. Testosterone for Life.
- Glaser RL, et al. Testosterone and Migraine Headaches: A Pilot Study. 2012;71(4):385–388.
- Glaser RL, York AE, Dimitrakakis C. Benefits of Testosterone Therapy in Women Measured by the Menopause Rating Scale. 2011;68(4):355–361.
- Burger HG, et al. Estradiol-Testosterone Implants in Menopausal Women: Clinical and Hormonal Outcomes. 1984;6(4):351.
🌿Your Next Step: Feel Like Yourself Again
Pellet therapy offers an elegant, effective way to restore hormone balance and optimize health. At Clearfield Medical Clinic, we guide you through every step—from labs to follow-ups—with care and expertise.
Ready to regain your spark?
Call us today at (775) 359-1222 or email cmg9550@gmail.com to schedule your consultation.